More debates over data but more focus on what data should be collected, the need for community consultation, and how it can and should be used:
As the Black Lives Matter movement spreads across Canada, the conversation around police accountability and reform has grown, including a rising interest in collecting more race-based data on people who interact with officers.
Adora Nwofor has been on the front lines with Black Lives Matter in Calgary. The activist and comedian says that if we do start collecting more race-based data, it’s important to make sure it helps the people it is supposed to help.
“If you want to collect race-based data, I very, very highly suggest that it is the populations that it affects that are getting that information first and then we are allowed to make suggestions as to what should be happening,” she said.
Earlier this year, Ontario became the first province to mandate all its police officers to identify and document the race of an individual on whom they have used force. This data collection initiative comes against the backdrop of large demonstrations against police violence in Canada, and the renewed focus on the policing of Black and Indigenous communities.
“By collecting disaggregated race data, you can provide a baseline for conversation. You can provide a baseline for creating a dialogue between police and the citizenry,” said Lorne Foster, a professor of public policy and human rights at York University in Toronto.
But not everyone thinks the goal of race data collection makes sense.
“I know for a fact that we’re victims, many people can say it, too.” said Samuel, a Black man from Montréal-Nord whose last name CBC has agreed not to publish because he fears harassment. His recent arrest during a traffic stop went viral after being videotaped.
“[The police] are going to try to show us what they want to show us, and not what we’re supposed to see.”
No charges were laid after Samuel’s traffic stop.
Foster was hired in 2013 by the City of Ottawa to design and study a race-based data collection project for police traffic stops. The project involved officers recording the race of the people they pulled over.
The pilot project was borne out of a human rights case involving a Black man who was stopped by police and alleged that he experienced racial profiling.
The data collected by the Ottawa police starting seven years ago showed that drivers who appeared to be Black or Middle Eastern were stopped at disproportionately higher rates.
The report found that in 2017-2018, “Middle Eastern drivers were stopped 3.18 times more than what you would expect based on their segment of the driving population while Black drivers were stopped 2.3 times more than what you would expect based on their population.”
‘This could be duplicated’
After the results were released, the police service created a multi-year action plan on diversity and inclusion in relation to the findings.
The Ottawa pilot is one of the few such initiatives in the country.
“We really do believe this could be duplicated in other municipalities across Canada,” Foster said.
In Ontario, since Jan. 1, 2020, officers have had to formally report the race of an individual in cases where they draw or fire a handgun, use a weapon other than a firearm on someone or are involved in a physical altercation with an individual that causes serious injuries requiring medical attention.
Officers must choose from a list of seven ethnic categories featured on what’s called a use of force report — a document that is filled out by police after such encounters.
The reports are sent to the Ministry of the Solicitor General, which oversees policing in the province, for analysis.
It’s part of Ontario’s Anti-Racism Act, which mandates race data collection “to identify and monitor systemic racism and racial disparities for the purpose of eliminating systemic racism and advancing racial equity.”
As of Jan. 1 of this year, Ontario police officers must choose from a list of seven ethnic categories when filling out a use of force report. (Ministry of the Solicitor General)
But while race-based data has been shown to help bring about reform, advocates are wary of how it will be used and caution against it as a one-stop solution to racial profiling.
“I think that before we continue to push for getting race-based data, we need to make some changes based on the information we already have,” said Nwofor.
“Quite frankly, I don’t need more race-based information next. I need change next. I need application of ideas from people who know that the police are systematically racist.”
It’s a perspective echoed by Myra Tait, an Indigenous lawyer and an instructor on Indigenous justice issues at the University of Winnipeg. Tait has studied how data and research are used in the justice system. While she sees benefits of race data collection and analysis, she said the process must happen in consultation with those the statistics affect.
“We have a very long history in this country of being studied and researched and having data collected on us, only to twist that around to blame the victim in a sense,” she said. “If you want to collect that data, then you do it with us. And you do it for us.”
Apart from Ontario, there are no provincewide mandates to collect race-based policing data. Some police services have taken on pilot projects to collect the data themselves in the past. Ottawa police are collecting the data for traffic stops, while Toronto and Halifax have collected data on street checks or police carding.
CBC News contacted Ontario’s 46 municipal police forces and the Ontario Provincial Police about how they are collecting and using race-based data.
Examining the data
While all of them have to send their reports to the province for analysis, some of them are also examining the data themselves. The extent of community engagement in the process is not clear in every case.
The Toronto Police Service, however, has put in place a race-based data collection strategy in order to prioritize community input, which has included four town halls, 51 focus groups and engagement with more than 800 residents.
“We asked them questions about our strategy: what they wanted to see from it, what did they think needed to be included in the training,” said Suelyn Knight, unit commander of the equity, inclusion and human rights section of the Toronto Police Service.
“It’s important for people to know that that’s also what’s fuelling our strategy, the voices from [the] community. And we’ll continue to do that. That was not a one-off.”
The Toronto race data collection initiative comes after controversies over racial profiling by the force, especially with regards to street checks, or police carding, of individuals.
In Nova Scotia, street checks were also controversial, and in fact were outlawed after a race-based data pilot project showed Black people were disproportionately targeted by Halifax police.
The analysis of data in that province is another example of race-based statistics leading to change, but it happened only after the public pressured the release of the data in 2017. Halifax police collected the data for years without making it public, and community consultation was missing from the equation.
Senator Wanda Thomas Bernard of Nova Scotia followed the debate over street checks in Halifax closely. While she sees the benefit from making the data public, she said a cautious approach is needed.
“It’s not just about collecting race-based data in policing, it’s really about what happens with that data,” Bernard said.
“Who owns the data? How is the community informed about this information? How is the information used to inform policies, but also to inform practices?”
The use of force reports currently ask the officer to record the race of people according to the officer’s perception. This raises questions about whether the information will be recorded correctly.
“How does an officer decide or distinguish what race the person is?” said Rob Davis, chief of police in Brantford, in southwestern Ontario.
“My fear is there is room for error or generalizing and may lead to false data and a ripple effect of misrepresentations.”
But it is the perception of the officer that’s important, said Foster, who worked on the Ottawa study.
“It’s not self-identified race that matters. It’s the other identified race that matters,” he said. “In other words, it’s the police that are doing the profiling. So it’s the police who interpret an individual’s race and act on that interpretation.”
Analysis coming next year
The Ontario Ministry of the Solicitor General says that currently, the Anti-Racism Act does not give them “the authority to collect self-identified race for use of force reports.” Police officers are “asked to give their best assessment of an individual’s race, honestly and in good faith. To identify and monitor the prevalence of racial bias or discrimination, it is important to capture perception.”
Ontario will analyze the race-based data every year, with the first release coming in 2021.
CBC News asked all other provinces and territories if they are planning to mandate race-based data collection for their police services. None had a plan like Ontario’s.
Alberta, for instance, said that data collection was up to local police services, but the province was planning to modernize its policing laws to make sure police are “accountable to the communities they protect.”
Saskatchewan does not have a provincial requirement for its police services either, but its police oversight body recently started collecting information on race on its complaint forms.
Others said it was up to the province or territory’s own police services or municipalities to collect the data if they wanted to.
While Australian approach to immigration is more restrictive than Canada’s, Canada’s economic and immigration recovery may also be longer than expected. But like all projections and estimates, time will tell.
Australia has been one of the more successful countries in addressing COVID-19, with only 311 infections and 4 deaths per million (July 1):
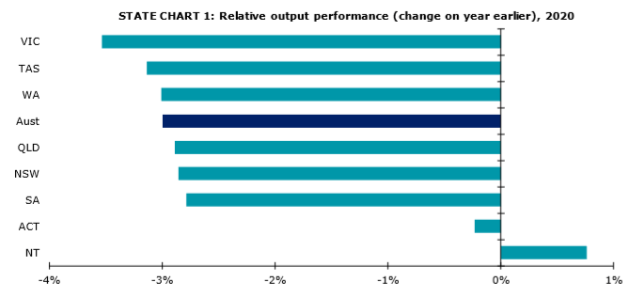
Australia’s second-most populous state was poised to take the biggest economic hit from the COVID-19 pandemic even before a dramatic spike in cases over the past fortnight forced renewed shutdowns in large parts of Melbourne.
Key points:
Victoria’s gross state product is expected to fall 1.6pc in 2020-21
The state is vulnerable due to its reliance on immigration from overseas and interstate
Many of the smaller states are expected to see higher peak unemployment rates, despite comparatively better economic performance
The latest business outlook from consultancy Deloitte Access Economics tips Victoria to suffer the biggest fall in gross state product in the 2020-21 financial year, which just began.
Deloitte predicts Victoria’s domestic economy will shrink 1.6 per cent this financial year, also leaving it with the worst economic performance in the nation this calendar year.
“The largest downturn is likely to be felt in Victoria given its current spike in cases, as well as that state’s dependence on migration and on foreign students in an age of lockdowns and closed borders,” Deloitte’s Chris Richardson said in the report.
Most state economies are expected to shrink around 3 per cent this year due to the pandemic.(Supplied: Deloitte)
Mr Richardson said Victoria’s economy was particularly vulnerable due to the latest wave of coronavirus cases, which would see the state cut off from the rest of the country, once the border with New South Wales closed from Wednesday.
“Victoria has had the strongest COVID restrictions across the country and now, with the prospect of a second wave returning and the reintroduction of restrictions, the state is likely to see some prolonged misery in particularly hard-hit sectors,” he noted.
Melbourne’s construction sector facing ‘severe setback’
While travel-related sectors, such as tourism and education, and hospitality will be the most immediate casualties, Mr Richardson says the medium-term effects will be felt acutely in the state’s previously booming construction sector.
“Victoria’s construction sector was already showing signs of weakness before COVID hit,” he wrote.
“With high levels of uncertainty, and an unexpected drop in population growth, construction is likely to suffer a severe setback over the coming year.
“Demand for office and apartments in Melbourne, including those projects that are halfway through, are being reconsidered as the density of Melbourne’s CBD is now less attractive across people’s daily lives.”
Mr Richardson added that one silver lining for Victoria’s construction sector was that there was a lot of planned infrastructure investment, something which would also be seen in the second-most pandemic-affected state, New South Wales.
It will particularly target transport projects in Melbourne and Sydney.
However, that investment is not expected to wholly make up for the loss of overseas arrivals.
“Other things equal, keeping tourists, students and migrants away for longer means that Australia’s economy will be some 4 to 5 per cent smaller than it could otherwise be,” Mr Richardson said.
Deloitte observed that New South Wales was similarly affected by the closure of international borders, with the state usually receiving more than a third of migrants who arrive in Australia from overseas.
However, in recent years, New South Wales has been losing existing residents to other Australian states, notably Victoria, a trend which Deloitte expects to have paused during the crisis, especially due to hard border closures.
The state’s comparatively better success in containing the virus so far has Deloitte tipping just a 0.1 per cent fall in New South Wales gross state product this financial year, as domestic activities continue to return to normal.
Some other states are expected to see a rise in their domestic activity — again excluding the large drop in exports, which includes foreign tourism and education — while the two territories are tipped to perform best.
“The lift in LNG-related exports from the Ichthys project will protect the Northern Territory, while its strong public sector base is a very welcome anchor in the storm for the ACT,” Mr Richardson explained.
Even though their domestic economies are expected to take a smaller hit than the bigger states, Deloitte is warning South Australia and Queensland will suffer the nation’s highest unemployment rates, above 9 per cent, while Western Australia and Tasmania will also have a weaker jobs market than Victoria.
Deloitte tips unemployment to be at its lowest in the ACT (5.7 per cent) and New South Wales (7.5 per cent).
COVID-19 infections ‘best’ economic indicator
Overall, Deloitte is forecasting a relatively fast recovery from the pandemic, tipping only a 0.4 per cent decline in GDP nationwide this financial year, following on from a 0.1 per cent fall in 2019-20.
It is predicting robust national economic growth of 5.3 per cent the following financial year, 2021-22.
However, this forecast is based on Australia keeping COVID-19 cases suppressed, a vaccine or good anti-viral treatments being widely available by the middle of next year, and international travel gradually recommencing, starting with trips to New Zealand at the end of this year and expanding to a general reopening of Australia’s borders by the end of next year.
Mr Richardson said a continued and widespread spike in cases would lead to much worse economic outcomes.
“That’s why opening up if virus numbers aren’t under control is risky.
“And, in a volatile environment, it is also why the best leading indicator of how an economy will perform is how that nation is going in its fight against the virus.”
Yet another Canadian advantage, short-lived should Trump be defeated:
Foreign students attending U.S. colleges that will operate entirely online this fall semester cannot remain in the country to do so, according to new regulations released Monday by U.S. Immigration and Customs Enforcement.
As college students across the United States and around the world contemplate what their upcoming semester might look like, the federal guidance limits options for international students and leaves them with an uncomfortable choice: attend in-person classes during a pandemic or take them online from another country.
And for students enrolled in schools that have already announced plans to operate fully online, there is no choice. Under the new rules, the State Department will not issue them visas, and U.S. Customs and Border Protection will not allow them to enter the country.
“Active students currently in the United States enrolled in such programs must depart the country or take other measures, such as transferring to a school with in-person instruction to remain in lawful status,” read a release from ICE’s Student and Exchange Visitor Program. “If not, they may face immigration consequences including, but not limited to, the initiation of removal proceedings.”
The agency said students already in the country and faced with a fully online course of study may take alternative measures to maintain their nonimmigrant status, “such as a reduced course load or appropriate medical leave.”
The rule applies to holders of F-1 and M-1 nonimmigrant visas, which allow nonimmigrant students to pursue academic and vocational coursework, respectively.
More than 1 million of the country’s higher education students come from overseas, according to the nonprofit Institute of International Education.
Typically, foreign students are limited in how many online courses they can take and are required to do the majority of their learning in the classroom, according to immigration lawyer Fiona McEntee. Once the pandemic struck, students were given flexibility to take more online classes — but only for the spring and summer semesters.
“It’s an unprecedented public health crisis, and I don’t think it’s too much to ask for the allowances that they made to continue, especially given the fact that we clearly, quite clearly do not have a handle on the pandemic here right now, unlike other countries that have,” McEntee said. “This makes no sense.”
McEntee said the decision is especially puzzling given the value of foreign students, which is quantifiable economically.
According to an economic analysis by NAFSA: Association of International Educators, international students studying at U.S. colleges and universities contributed $41 billion and supported 458,290 jobs during the 2018-2019 academic year.
McEntee added that losing foreign students is a huge blow to university budgets, something that will impact domestic students as well. Similarly, the decision to attend classes in person impacts all students present.
“If students can study online successfully from an academic point of view, why are we forcing them to come into a situation where they could put their health at risk and also the health of their classmates at risk?” she asked.
Students attending schools operating as usual will remain bound by existing federal regulations that permit them to take a maximum of one class or three credit hours online.
Students attending schools implementing a hybrid model can take more online classes or credits, though their school must certify “that the program is not entirely online, that the student is not taking an entirely online course load this semester, and that the student is taking the minimum number of online classes required to make normal progress in their degree program.”
The announcement comes as higher education institutions are releasing frameworks for reopening in the fall semester. Schools are preparing to offer in-person instruction, online classes or a mix of both.
Eight percent of colleges are planning to operate online, according to the Chronicle of Higher Education, which is tracking the reopening plans of more than 1,000 U.S. colleges. Sixty percent are planning for in-person instruction, and 23% are proposing a hybrid model, with a combined 8.5% undecided or considering a range of scenarios.
Harvard University is one of the latest institutions to unveil its plans, announcing on Monday that all undergraduate and graduate course instruction for the academic year will be held online. Nevertheless, the university plans to bring 40% of undergraduates, including all freshmen, onto campus.
Harvard President Larry Bacow said in a statement emailed to NPR that the ICE policy is “a blunt, one-size-fits-all approach to a complex problem.”
“We must do all that we can to ensure that our students can continue their studies without fear of being forced to leave the country mid-way through the year, disrupting their academic progress and undermining the commitments—and sacrifices—that many of them have made to advance their education,” the statement said.
School reopening plans may be subject to change because of the evolving nature of the pandemic, especially with daily case totals continuing to break records in parts of the country.
In acknowledgment, the agency instructs schools to update their information in the Student and Exchange Visitor Information System within 10 days of making the switch to online-only classes.
Immigration lawyer McEntee, a former international student herself, said leaving for school can be challenging enough, not to mention during a pandemic and in a landscape of near-constant immigration restrictions. She called the new rule, both in substance and timing, “not right.”
“This is not the America that I think foreign students come to live in,” she said.
The American Council on Education, a higher education lobbying group, also condemned the rule change in a statement issued Monday afternoon. ACE President Ted Mitchell said the guidance “provides confusion and complexity rather than certainty and clarity” and called on ICE to rethink its position.
“At a time when institutions are doing everything they can to help reopen our country, we need flexibility, not a big step in the wrong direction,” he wrote. “ICE should allow any international student with a valid visa to continue their education regardless of whether a student is receiving his or her education online, in person, or through a combination of both, whether in the United States or in their home country, during this unprecedented global health crisis.”
Interesting study and findings, including what appear to be reasonable explanations for these findings. Most health-related studies of immigrants tend to highlight health disparities between immigrants and non-immigrants and the adverse effects of Canadian diets on immigrants over time:
Anxiety disorders are among the most commonly diagnosed disabilities around the globe. Previous research suggests that the risk for anxiety disorders varies according to demographic, socio-economic, and health-related factors. Interestingly, despite the fact that immigrants face certain hardships and unique disadvantages compared to nonimmigrants, new research has found that immigrants show lower rates of anxiety.
“Our research team is interested in analyzing Canadian Longitudinal Study on Aging data to examine factors which affect mental health,” said Karen Davison, North American Primary Care Research Group Fellow and Health Science Program Chair at Kwantlen Polytechnic University in Surrey, who led the study.
“Given that anxiety disorders have such a high global burden related to disability, we were particularly interested in examining various social, economic, health, and nutrition-related factors and their relationships with the condition. This information could help to improve health practices, programs, and policies for adults.”
Davison and her team conducted a study to explore the relationship between immigrant status and anxiety disorders with a focus on older adults. They further explored nutritional and health-related factors that might mitigate the risk for anxiety disorders among all Canadians.
The researchers analyzed baseline data from the ongoing Canadian Longitudinal Study on Aging, resulting in a sample of 26,991 Canadian residents between the ages of 45-85. The survey measured self-reported lifetime anxiety disorder with the question, “Has a doctor ever told you that you have an anxiety disorder such as a phobia, obsessive-compulsive disorder or a panic disorder?” The study also included various demographic, economic, health, and nutritional measures.
Across the sample, 8.5% of respondents reported being diagnosed with an anxiety disorder at some point in their lifetime. Interestingly, while 9% of Canadian-born respondents reported an anxiety diagnosis, only 6% of immigrants did. When accounting for age and sex, this represented 30% lower odds of being diagnosed with anxiety for immigrants.
The authors offered several explanations for what researchers call the “healthy immigrant effect.” Canada uses a points-based immigration system, which classifies a person’s eligibility to immigrate to Canada according to their skills and qualifications. Those accepted to immigrate generally have a higher education and better work experience, qualities that may lessen their susceptibility to anxiety disorders.
“Another potential explanation … is that potential immigrants with anxiety disorders would find the challenges of relocation too anxiety inducing and would therefore not choose to immigrate,” the authors wrote.
Certain health factors impacted the likelihood of an anxiety disorder diagnosis. Having at least one existing health condition, experiencing chronic pain, being categorized as underweight, having a higher percentage of body fat, or smoking 100 or more cigarettes over one’s lifetime were each associated with increased odds of being diagnosed with anxiety.
Nutritional factors also impacted reports of anxiety. Across the sample, those who consumed two or more fiber sources a day or one or more pastries a day were more likely to be diagnosed with an anxiety disorder. Alternatively, those who consumed 0.5 to 2 sources of pulses and nuts per day or three or more sources of fruit and vegetables per day were less likely to have anxiety. This may be because fruits, vegetables, and nuts contain high levels of zinc, magnesium, and vitamin B, which have been associated with reduced anxiety.
“We believe the main message of this study is that after accounting for many social, economic, health, and nutrition-related factors, a significant relationship was found between fruit and vegetable intakes and having been diagnosed with an anxiety disorder. It is well established that fruit and vegetable intakes are associated with physical health. This study lends to the increasing evidence that shows there are also links with mental health,” Davison told PsyPost.
“In this study we found that lower intakes of calcium rich foods with high vitamin D content are associated with lower odds of anxiety disorders. However, as the number of sources consumed increased, the trends in the odds ratios showed what seemed to be a positive or dose-response type relationship. For future studies we would like to examine supplement sources of calcium and vitamin D which are commonly taken by older adults and their relationship with anxiety disorders. In addition, for future work we plan to examine biomarkers and genomic markers related to calcium and vitamin D which may help us to better understand these relationships.”
“Another finding we would like to highlight is the associations we found with higher percent body fat and anxiety. This relationship may be due to mechanisms related to immune-inflammatory activation. Previous research has shown that individuals with high body fat and mental ill health have increased inflammatory markers, such as C-reactive protein, interleukin-6, and tumour necrosis factor-alpha. The activation of certain immune system cells in response to ongoing chronic inflammation, has been linked with poor mental health. Certainly more research is needed to better understand the possible links between body composition and anxiety,” Davison added.
The authors concluded that their findings offer insight into nutritional, health-rated, and social factors associated with anxiety disorder diagnoses among immigrants and Canadian-born residents of Canada. These insights could help inform treatment for middle age and older adults with anxiety.
Apart from the somewhat polemic introduction, a good discussion of the limits of aggregated visible minority groups and the need for more desegregated data by country of ethnic ancestry (rather than nationality, given need to include second and subsequent generations).
However, starting with the basic visible minority data, which could then be matched with census socio-economic data, is a needed start to further needed disaggregation:
All over the world, the COVID-19 pandemic has disproportionately affected patients based on a variety of identifiable factors, from age to sex to occupation. Data such as these are crucial to public-health officials and researchers tasked with improving care for all citizens. But in some cases, the quest for data seems driven as much by political factors as by the need to protect public health.
In Canada, where I work as a resident physician in the field of head and neck surgery, the federal government has proposed that racial data be tracked as part of our national response to the COVID-19 pandemic, as is already the case in the United States. On the surface, there would seem to be an obvious parallel with the need to collect race-based policing data, especially in the wake of George Floyd’s death and the worldwide protests that followed.
Collecting such data makes sense in the context of policing, since race corresponds to a visible marker that can prompt radically different responses from police officers. But the situation is different when it comes to public health. And using race as a proxy for socioeconomic and environmental explanations of disease—by broadly categorizing patients as White, Black, Asian, Indigenous, and so on, according to melanin-influenced phenotype—is a dangerous leap. Obtaining more detailed data, including nationality-based information, would be a more fruitful endeavor.
Consider the use of broad racial typologies in the field of education. York University professors Carl James and Tana Turner combed through Toronto District School Board data to go beyond the officially recognized categories of “Black” and “White.” In so doing, they discovered that recent immigrants from Africa and the Caribbean tend to perform better than those with generational ties to Canada. This disparity is not evident within the aggregated statistics, wherein both of these groups are simply classified as Black. In a country with a rich recent history of immigration, such as Canada, finer distinctions are particularly important.
Similar examples arise when it comes to race-based health data. Sickle cell anemia, a blood disease with a challenging clinical trajectory, is most commonly found in sub-Saharan Africa, whose population undeniably may be placed within the “Black” designation. But examining sub-populations within this category yields surprising trends. Sickle cell anemia is about 100 times more common in Nigeria than in Somalia. Making matters more confusing, the prevalence of the disease is higher in Greece, whose majority population we may safely place in the “White” category, than in either Somalia or Jamaica. Terms such as “Black” and “White” simply become useless when talking about many areas of health-related statistics.
In some rare instances, there may be a direct causal association between skin melanin content and disease. Skin cancers fall into this category. Here, we may confidently assert that racial characteristics are relevant to the biological explanation for the disease. Medicine has long recognized this, and has adapted to it—including through the so-called Fitzpatrick scale as a tool to help evaluate risk based on skin tone.
In the case of COVID-19, we know that diabetes, hypertension, and obesity all are significant comorbidities. Does skin melanin content have an effect on incidence rates and mortality? We can’t confidently come to a conclusion one way or another. But any clinician will tell you that such a link is improbable. Yes, there are outcome disparities that align with race. But such disparities among racialized Canadian communities seem largely related to unequal access to care, and to socioeconomic factors related to a historical narrative of inequality. Those inequalities should be addressed regardless of whether they manifest themselves in COVID-19 data.
Broad categorizations fall apart when it comes to Indigenous groups as well. It is no secret that Indigenous Canadians face unacceptable health disparities when compared to non-Indigenous Canadians. By many accounts, the state of Indigenous health in Canada is a shameful stain on an otherwise successful universal healthcare enterprise. But just as with Somali-Canadians and Greek-Canadians, each Indigenous community faces unique challenges related to their disease burden. While arthritis and rheumatism are more common amongst Indigenous groups as a whole, the prevalence of these conditions is significantly higher for First Nations as compared to Inuit communities in the northern part of the country. Surely this is important when determining priorities in a cash-strapped healthcare delivery environment.
Similarly, a sub-group analysis reveals that northern Inuit communities in Nunavut and the Northwest Territories face significantly greater challenges related to access to care as compared to First Nations people in the provinces, who are more likely to live closer to large hospitals and specialist medical clinics. These disparities are a matter of geography, amongst other things. Yet important patterns are masked if the data is simply grouped under broad categories such as “Indigenous” and “Non-Indigenous.”
These examples underscore the need for granularity in data collection. More detailed information encompassing nationality and background, in combination with other important socio-economic factors, allow for a more complete picture of the health problems that must be addressed. There are numerous health-outcome disparities between “Black” and “White” Canadians that many politicians and policy makers, with good intentions, seek to cast as evidence of systemic racism. Putting aside how that term should be defined, such an approach would apply a misguided oversimplification to the practice of medical data collection.
The goal should be to help all Canadians—especially those who truly need it. Statements such as “Canadian females of Filipino descent have higher incidence rates of thyroid cancer when compared to the general population” are much more useful than “Asian-Canadian females have higher rates of thyroid cancer.” That is why Public Health Ontario and organizations such as the ICES research institute already use large data sets to fine-tune clinical practices and improve the livelihood of all citizens.
Thanks to advances in machine learning, we have the tools to collect, store, and analyze data on an even larger scale. But our efforts will be successful only if we apply a typology that is based on categories useful to doctors and patients, not politicians and activists.
Good nuanced discussion, based upon US experience but likely also applicable here:
As the pandemic took hold, most epidemiologists have had clear proscriptions in fighting it: No students in classrooms, no in-person religious services, no visits to sick relatives in hospitals, no large public gatherings.
So when conservative anti-lockdown protesters gathered on state capitol steps in places like Columbus, Ohio and Lansing, Mich., in April and May, epidemiologists scolded them and forecast surging infections. When Gov. Brian Kemp of Georgia relaxed restrictions on businesses in late April as testing lagged and infections rose, the talk in public health circles was of that state’s embrace of human sacrifice.
And then the brutal killing of George Floyd by police in Minneapolis on May 25 changed everything.
Soon the streets nationwide were full of tens of thousands of people in a mass protest movement that continues to this day, with demonstrations and the toppling of statues. And rather than decrying mass gatherings, more than 1,300 public health officials signed a May 30 letter of support, and many joined the protests.
That reaction, and the contrast with the epidemiologists’ earlier fervent support for the lockdown, gave rise to an uncomfortable question: Was public health advice in a pandemic dependent on whether people approved of the mass gathering in question. To many, the answer seemed to be, “Yes.”
“The way the public health narrative around coronavirus has reversed itself overnight seems an awful lot like … politicizing science,” the essayist and journalist Thomas Chatterton Williams wrote in The Guardian last month. “What are we to make of such whiplash-inducing messaging?”
Of course, there are differences: A distinct majority of George Floyd protesters wore masks in many cities, even if they often crowded too close together. By contrast, many anti-lockdown protesters refused to wear masks — and their rallying cry ran directly contrary to public health officials’ instructions.
And in practical terms, no team of epidemiologists could have stopped the waves of impassioned protesters, any more than they could have blocked the anti-lockdown protests.
Still, the divergence in their own reactions left some of the country’s prominent epidemiologists wrestling with deeper questions of morality, responsibility and risk.
Catherine Troisi, an infectious disease epidemiologist at The University of Texas Health Science Center at Houston, studies Covid-19. When, wearing a mask and standing at the edge of a great swell of people, she attended a recent protest in Houston supporting Mr. Floyd, a sense of contradiction tugged at her.
“I certainly condemned the anti-lockdown protests at the time, and I’m not condemning the protests now, and I struggle with that,” she said. “I have a hard time articulating why that is OK.”
Mark Lurie, a professor of epidemiology at Brown University, described a similar struggle.
“Instinctively, many of us in public health feel a strong desire to act against accumulated generations of racial injustice,” Professor Lurie said. “But we have to be honest: A few weeks before, we were criticizing protesters for arguing to open up the economy and saying that was dangerous behavior.
“I am still grappling with that.”
To which Ashish Jha, dean of Brown University’s School of Public Health, added: “Do I worry that mass protests will fuel more cases? Yes, I do. But a dam broke, and there’s no stopping that.”
Some public health scientists publicly waved off the conflicted feelings of their colleagues, saying the country now confronts a stark moral choice. The letter signed by more than 1,300 epidemiologists and health workers urged Americans to adopt a “consciously anti-racist” stance and framed the difference between the anti-lockdown demonstrators and the protesters in moral, ideological and racial terms.
Those who protested stay-at-home orders were “rooted in white nationalism and run contrary to respect for Black lives” the letter stated.
By contrast, it said, those protesting systemic racism “must be supported.”
“As public health advocates,” they stated, “we do not condemn these gatherings as risky for Covid-19 transmission. We support them as vital to the national public health.”
There is as of yet no firm evidence that protests against police violence led to noticeable spikes in infection rates. A study published by the National Bureau of Economic Research found no overall rise in infections, but could not rule out that infections might have risen in the age demographic of the protesters. Health officials in Houston and Los Angeles have suggested the demonstrations there led to increased infections, but they have not provided data. In New York City, Mayor Bill de Blasio has instructed contact tracers not to ask if infected people attended protests.
The ten epidemiologists interviewed for this article said near-daily marches and rallies are nearly certain to result in some transmission. Police use of tear gas and pepper spray, and crowding protesters into police vans and buses, puts people further at risk.
“In all likelihood, some infections occurred at the protests; the question is how much,” said Professor Lurie. “No major new evidence has emerged that suggests the protests were superspreader events.”
The coronavirus has infected 2.89 million Americans, and at least 129,800 have died.
The virus has hit Black and Latino Americans with a particular ferocity, hospitalizing those populations at more than four times the rate of white Americans. Many face underlying health issues, and are more likely than most Americans to live in densely populated housing and to work on the front lines of this epidemic. As a result, Latinos and Black people are dying at rates well in excess of white Americans.
Mary Travis Bassett, who is African American, served as the New York City health commissioner and now directs the FXB Center for Health and Human Rights at Harvard University. She noted that even before Covid-19, Black Americans were sicker and died more than two years earlier, on average, than white Americans.
And she noted, police violence has long cast a deep shadow over African Americans. From the auction block to plantations to centuries of lynchings carried out with the complicity of local law enforcement, blacks have suffered the devastating effects of state power.
She acknowledged that the current protests are freighted with moral complications, not least the possibility that a young person marching for justice might come home and inadvertently infect a mother, aunt or grandparent. “If there’s an elder in the household, that person should be cocooned to the best extent that we can,” Professor Bassett said.
But she said the opportunity to achieve a breakthrough transcends such worries about the virus. “Racism has been killing people a lot longer than Covid-19,” she said. “The willingness to say we all bear the burden of that is deeply moving to me.”
Others take a more cautious view of the moral stakes. Nicholas A. Christakis, professor of social and natural science at Yale, noted public health is guided by twin imperatives: To comfort the afflicted and to speak truth about risks to public health, no matter how unpleasant.
These often-complementary values are now in conflict. To take to the street to protest injustice is to risk casting open doors and letting the virus endanger tens of thousands, he said. There is a danger, he said, in asserting that one moral imperative overshadows another.
“The left and the right want to wish the virus away,” Professor Christakis said. “We can’t wish away climate change, or the epidemic, or other inconvenient scientific truths.”
He said that framing the anti-lockdown protests as white supremacist and dangerous and the George Floyd protests as anti-racist and essential obscures a messier reality.
When he was a hospice doctor in Chicago and Boston, he said, he saw up close how isolation deepened the despair of the dying — a fate now suffered by many in the pandemic, with hospital visits severely restricted. For epidemiologists to turn around and argue for loosening the ground rules for the George Floyd marches risks sounding hypocritical.
“We allowed thousands of people to die alone,” he said. “We buried people by Zoom. Now all of a sudden we are saying, never mind?”
There are other conflicting imperatives. Lockdowns, and the shuttering of businesses and schools and enforcing social isolation, take a toll on the working class and poor, and the emotionally fraught who live on the economic margins.
The lockdown is justified, most epidemiologists say, even as it requires acknowledging a moral truth: To save many hundreds of thousands of lives, we risk wrecking the lives of a smaller number of Americans, as businesses fail and people lose jobs and grow desolate and depressed.
The pandemic has also brought an increase in deaths from heart attacks and diabetes during this period.
“Have people died because of the closed economy? No doubt,” said Professor Lurie, the Brown University epidemiologist. “And that pain is real, and should not be dismissed. But you won’t have a healthy economy until you have healthy people.”
There’s another epidemiological reality: No one quite understands the path of this idiosyncratic virus and how and when it strikes. The public health risks presented by the protests are not easily separated from the broader risks taken as governors, in fits and starts, move to reopen state economies. The protesters represent a small stream filled with 500,000 to perhaps 800,000 people, merging with a river of millions of Americans who have begun to re-enter businesses and restaurants.
“To separate out those causes, when we look, will be very difficult,” Professor Lurie noted.
Still, he admitted to some worries. He said he took his daughter to a protest early in June and felt a chaser of regret in its wake.
“We felt afterward that the risk we incurred probably exceeded the entire risk in the previous two months,” he said. “We undid some very hard work, and I don’t see how actions like that can help in battling this epidemic, honestly.”
Good in-depth analysis (for charts, see the article):
Teresa and Marvin Bradley can’t say for sure how they got the coronavirus. Maybe Ms. Bradley, a Michigan nurse, brought it from her hospital. Maybe it came from a visiting relative. Maybe it was something else entirely.
What is certain — according to new federal data that provides the most comprehensive look to date on nearly 1.5 million coronavirus patients in America — is that the Bradleys are not outliers.
Racial disparities in who contracts the virus have played out in big cities like Milwaukee and New York, but also in smaller metropolitan areas like Grand Rapids, Mich., where the Bradleys live. Those inequities became painfully apparent when Ms. Bradley, who is Black, was wheeled through the emergency room.
“Everybody in there was African-American,” she said. “Everybody was.”
Early numbers had shown that Black and Latino people were being harmed by the virus at higher rates. But the new federal data — made available after The New York Times sued the Centers for Disease Control and Prevention — reveals a clearer and more complete picture: Black and Latino people have been disproportionately affected by the coronavirus in a widespread manner that spans the country, throughout hundreds of counties in urban, suburban and rural areas, and across all age groups.
Latino and African-American residents of the United States have been three times as likely to become infected as their white neighbors, according to the new data, which provides detailed characteristics of 640,000 infections detected in nearly 1,000 U.S. counties. And Black and Latino people have been nearly twice as likely to die from the virus as white people, the data shows.
The disparities persist across state lines and regions. They exist in rural towns on the Great Plains, in suburban counties, like Fairfax County, Va., and in many of the country’s biggest cities.
“Systemic racism doesn’t just evidence itself in the criminal justice system,” said Quinton Lucas, who is the third Black mayor of Kansas City, Mo., which is in a state where 40 percent of those infected are Black or Latino even though those groups make up just 16 percent of the state’s population. “It’s something that we’re seeing taking lives in not just urban America, but rural America, and all types of parts where, frankly, people deserve an equal opportunity to live — to get health care, to get testing, to get tracing.”
The data also showed several pockets of disparity involving Native American people. In much of Arizona and in several other counties, they were far more likely to become infected than white people. For people who are Asian, the disparities were generally not as large, though they were 1.3 times as likely as their white neighbors to become infected.
The new federal data, which is a major component of the agency’s disease surveillance efforts, is far from complete. Not only is race and ethnicity information missing from more than half the cases, but so are other epidemiologically important clues — such as how the person might have become infected.
And because it includes only cases through the end of May, it doesn’t reflect the recent surge in infections that has gripped parts of the nation.
Still, the data is more comprehensive than anything the agency has released to date, and The Times was able to analyze the racial disparity in infection rates across 974 counties representing more than half the U.S. population, a far more extensive survey than was previously possible.
Disparities in the suburbs
For the Bradleys, both in their early 60s, the symptoms didn’t seem like much at first. A tickle at the back of the throat.
But soon came fevers and trouble breathing, and when the pair went to the hospital, they were separated. Ms. Bradley was admitted while Mr. Bradley was sent home. He said he felt too sick to leave, but that he had no choice. When he got home, he felt alone and uncertain about how to treat the illness.
It took weeks, but eventually they both recovered. When Mr. Bradley returned to work in the engineering department of a factory several weeks later, a white co-worker told Mr. Bradley that he was the only person he knew who contracted the virus.
By contrast, Mr. Bradley said he knew quite a few people who had gotten sick. A few of them have died.
“We’re most vulnerable to this thing,” Mr. Bradley said.
In Kent County, which includes Grand Rapids and its suburbs, Black and Latino residents account for 63 percent of infections, though they make up just 20 percent of the county’s population. Public health officials and elected leaders in Michigan said there was no clear reason Black and Latino people in Kent County were even more adversely affected than in other parts of the country.
Among the 249 counties with at least 5,000 Black residents for which The Times obtained detailed data, the infection rate for African-American residents is higher than the rate for white residents in all but 14 of those counties. Similarly, for the 206 counties with at least 5,000 Latino residents analyzed by The Times, 178 have higher infection rates for Latino residents than for white residents.
“As an African-American woman, it’s just such an emotional toll,” said Teresa Branson, the deputy administrative health officer in Kent County, whose agency has coordinated with Black pastors and ramped up testing in hard-hit neighborhoods.
Experts point to circumstances that have made Black and Latino people more likely than white people to be exposed to the virus: Many of them have front-line jobs that keep them from working at home; rely on public transportation; or live in cramped apartments or multigenerational homes.
“You literally can’t isolate with one bathroom,” said Lt. Gov. Garlin Gilchrist II, who leads Michigan’s task force on coronavirus racial disparities.
‘We just have to keep working’
Latino people have also been infected at a jarringly disparate rate compared with white people. One of the most alarming hot spots is also one of the wealthiest: Fairfax County, just outside of Washington, D.C.
Three times as many white people live there as Latinos. Yet through the end of May, four times as many Latino residents had tested positive for the virus, according to the C.D.C. data.
Diana, who is 26 and did not want her last name used out of fear for her husband’s job, said her husband got sick at a construction site in April. She and her brother, who also works construction, soon fell ill, too. With three children between them, the six family members live in a two-bedroom apartment.
Diana, who was born in the United States but moved to Guatemala with her parents as a small child before returning to this country five years ago, is still battling symptoms. “We have to go out to work,” she said. “We have to pay our rent. We have to pay our utilities. We just have to keep working.”
At Culmore Clinic, an interfaith free clinic serving low-income adults in Fairfax, about half of the 79 Latino patients who tested for the virus have been positive.
“This is a very wealthy county, but their needs are invisible,” said Terry O’Hara Lavoie, a co-founder of the clinic. The risk of getting sick from tight living quarters, she added, is compounded by the pressure to keep working or quickly return to work, even in risky settings.
The risks are borne out by demographic data. Across the country, 43 percent of Black and Latino workers are employed in service or production jobs that for the most part cannot be done remotely, census data from 2018 shows. Only about one in four white workers held such jobs.
Also, Latino people are twice as likely to reside in a crowded dwelling — less than 500 square feet per person — as white people, according to the American Housing Survey.
The national figures for infections and deaths from the virus understate the disparity to a certain extent, since the virus is far more prevalent among older Americans, who are disproportionately white compared with younger Americans. When comparing infections and deaths just within groups who are around the same ages, the disparities are even more extreme.
Latino people between the ages of 40 and 59 have been infected at five times the rate of white people in the same age group, the new C.D.C. data shows. The differences are even more stark when it comes to deaths: Of Latino people who died, more than a quarter were younger than 60. Among white people who died, only 6 percent were that young.
Jarvis Chen, a researcher and lecturer at the Harvard T. H. Chan School of Public Health, said that the wide racial and ethnic disparities found in suburban and exurban areas as revealed in the new C.D.C data should not come as a surprise. The discrepancies in how people of different races, ethnicities and socioeconomic statuses live and work may be even more pronounced outside of urban centers than they are in big cities, Dr. Chen said.
“As the epidemic moves into suburban areas, there are good reasons to think that the disparities will grow larger,” he said.
The shortfalls of the government’s data
The Times obtained the C.D.C. data after filing a Freedom of Information Act lawsuit to force the agency to release the information.
To date, the agency has released nearly 1.5 million case records. The Times asked for information about the race, ethnicity and county of residence of every person who tested positive, but that data was missing for hundreds of thousands of cases.
C.D.C. officials said the gaps in their data are because of the nature of the national surveillance system, which depends on local agencies. They said that the C.D.C. has asked state and local health agencies to collect detailed information about every person who tests positive, but that it cannot force local officials to do so. Many state and local authorities have been overwhelmed by the volume of cases and lack the resources to investigate the characteristics of every individual who falls ill, C.D.C. officials said.
Even with the missing information, agency scientists said, they can still find important patterns in the data, especially when combining the records about individual cases with aggregated data from local agencies.
Still, some say the initial lack of transparency and the gaps in information highlight a key weakness in the U.S. disease surveillance system.
“You need all this information so that public health officials can make adequate decisions,” said Andre M. Perry, a fellow in the Metropolitan Policy Program at The Brookings Institution. “If they’re not getting this information, then municipalities and neighborhoods and families are essentially operating in the dark.”
Higher cases, higher deaths
The higher rate in deaths from the virus among Black and Latino people has been explained, in part, by a higher prevalence of underlying health problems, including diabetes and obesity. But the new C.D.C. data reveals a significant imbalance in the number of virus cases, not just deaths — a fact that scientists say underscores inequities unrelated to other health issues.
The focus on comorbidities “makes me angry, because this really is about who still has to leave their home to work, who has to leave a crowded apartment, get on crowded transport, and go to a crowded workplace, and we just haven’t acknowledged that those of us who have the privilege of continuing to work from our homes aren’t facing those risks,” said Dr. Mary Bassett, the Director of the FXB Center for Health and Human Rights at Harvard University.
Dr. Bassett, a former New York City health commissioner, said there is no question that underlying health problems — often caused by factors that people cannot control, such as lack of access to healthy food options and health care — play a major role in Covid-19 deaths.
But she also said a big determinant of who dies is who gets sick in the first place, and that infections have been far more prevalent among people who can’t work from home. “Many of us also have problems with obesity and diabetes, but we’re not getting exposed, so we’re not getting sick,” she said.
The differences in infection case rates are striking, said Jennifer Nuzzo, an epidemiologist and professor at the Johns Hopkins Bloomberg School of Public Health.
“Some people have kind of waved away the disparities by saying, ‘Oh, that’s just underlying health conditions,’” Dr. Nuzzo said. “That’s much harder to do with the case data.”
In June, C.D.C. officials estimated that the true tally of virus cases was 10 times the number of reported cases. They said they could not determine whether these unreported cases had racial and ethnic disparities similar to those seen in the reported infections.
But they said that more-severe infections — which are more often associated with underlying health conditions, and with people seeking medical care — are more likely to be recorded as cases.
That difference in the reporting of cases might explain some portion of the race and ethnicity disparities in the number of documented infections, C.D.C. officials said. But they said that it was also clear that there have been significant disparities in the number of both deaths and cases.
Donald Trump’s June 22, 2020, presidential proclamationappeared aimed at preventing the entry of foreign workers. However, the proclamation had another, equally important target – spouses and children.
Why would Trump and his team try to prevent the entry of spouses and children in a proclamation whose stated purpose was to “protect unemployed Americans”? The answer lies in the administration’s policy of separating Central American families who crossed the U.S. border, which took public anger over recordings of crying children being held in detention facilities to end.
In October 2018, Donald Trump made his intentions in separating children at the border from family members clear. “We have people trying to come in like never before,” said Trump. “If they feel there will be separation, then they won’t come.”
A similar logic seems behind the presidential proclamation. Catherine Rampell, a columnist for the Washington Post, recently wrote about Vihaan Baranidharan, who is 7-years-old: “Vihaan is stuck in India, where he went to see his sick grandmother for what was supposed to be a short visit. Thanks to Trump’s order, he’s blocked from getting the visa stamp needed to return to Dallas. But Vihaan has not taken, nor has any plans to take, any American’s job . . . Vihaan just finished first grade.”
The text of the proclamation singles out spouses and children as a “threat,” which means preventing 7-year-olds from joining their mothers or fathers in America was an intended, not an unintended, consequence. The proclamation reads: “Temporary workers are often accompanied by their spouses and children, many of whom also compete against American workers.” As attorneys point out, the phrase “many of whom” is not true, even if one believed in the “lump of labor fallacy,” the discredited notion that there is a fixed quantity of labor needed in an economy on which the presidential proclamation is based.
“The universe of spouses and children entitled to work authorization in the U.S. is rather limited, so there’s scant economic rationale for barring them from entry,” said Vic Goel, managing partner of Goel & Anderson, in an interview. “Only spouses of L-1 and J-1 nonimmigrants are automatically entitled to apply for work authorization in the U.S, and spouses of H-1B workers qualify only when the principal H-1B worker has been approved or has experienced significant government delay for an application leading to permanent residence. Dependent spouses and children of H-2B workers are barred from working in the U.S., as are the children of H-1B and L-1 visa holders.” He also points out even if arriving dependents were eligible for work authorization, they would be unlikely to get approved before the end of the year.
After the harmful effects on families became publicly known, the Trump administration amended the proclamation to make it more restrictive. “Under the language of the original provision, having a valid visa of any category was sufficient to exempt an individual from the proclamation,” writes attorney Cyrus Mehta. “The amendment renders the proclamation even more restrictive, specifying that the visa must be a valid H-1B, H-2B, L, or certain J visas, and that the individual must be entering the United States pursuant to that visa to qualify for an exemption. . . . . Already, the proclamation is resulting in irreparable harm and separated families.”
Attorney Greg Siskind thinks families were targeted because Section 212(f) of the Immigration and Nationality Act, the authority used in the proclamation, limits the president’s power to restricting entry. He believes the more restrictive interpretation of the proclamation and the language on families allows the administration to go after people inside the country. “In effect, they’re forcing people to self-deport because they have found a permanent way to keep families separated,” he told me.
By “permanent,” Siskind refers to the open-ended nature of the proclamation, which “ends” on December 31, 2020, but could continue for an additional 4 years beyond that date if Donald Trump is reelected and no court limits the proclamation’s scope. Siskind expects foreign governments to retaliate against U.S. companies and their operations overseas if employees of multinational companies continue to be prohibited from entering the United States to work. (The proclamation prevents L visa holders from transferring into the United States.)
Jeffrey Gorsky of Berry, Appleman & Leiden believes that by including children, as well as spouses who are ineligible to work, the administration made the proclamations (of April 22, 2020, and June, 22, 2020) more vulnerable to legal challenge, since the alleged reason for the proclamations were economic.
He also points out the perverse, some might even say cruel, impact of the administration’s actions. He gives the example of an L visa holder “stuck in Europe because of another travel ban currently in place that bars anyone physically present in the Schengen region from coming to the U.S. unless they have been outside that region for 14 days.” Although as a current visa holder the woman would be exempt from the proclamation, that would not be the case for a child if she gives birth. “The newborn child will be subject to the new travel ban because, unlike the child’s mother, the child will not have a visa valid at the time of the effective date of the ban,” according to Gorsky. “As a result, the mother can return to her employment in the U.S., but the infant is barred from the U.S. on the legal grounds that the infant’s admission would be detrimental to the interests of the U.S. as a threat to U.S. employment.”
In addition to the proclamation, the Trump administration has promised to rescind the regulation that allows the spouses of H-1B visa holders to receive employment authorization documents (EADs); 93% of the spouses on EADs are women. The work authorization makes it easier for H-1B families to bear the long wait for employment-based green cards, which is what appears to have motivated administration officials to eliminate it.
A possible plan suggested in the June 22, 2020, proclamation could drive hundreds of thousands of long-time H-1B visa holders out of the United States. The plan, if the administration pursues it, would compel foreign nationals waiting years for employment-based green cards to go through “labor certification” again – a process in most cases completed years earlier – in the hopes many will not succeed, particularly if the administration changes the process to make it more difficult. Failure to pass a second labor certification could force H-1B visa holders waiting for green cards to leave the country.
“By barring spouses and children from entry when the principal temporary visa holder is already in the U.S., the proclamation inflicts much pain and suffering on those workers,” said Vic Goel. “It presents them with a choice of continuing their employment in the U.S. or leaving the country to be reunited with their family members.”
It appears those running U.S. immigration policy today do not believe it is sufficient to keep out highly skilled professionals, despite the economic cost to the nation. The evidence indicates Trump administration officials also want to drive out foreign-born scientists and engineers currently working in the United States. Separating high-skilled foreign nationals from their spouses and children as another way to achieve this goal is not only acceptable to administration officials, analysts note, it’s been planned out. As Donald Trump said about desperate Central American parents: “If they feel there will be separation, then they won’t come.”
Well, we will know for sure this summer, the peak period for arrivals.
But an interesting snapshot of intentions, carried out by Ka Ho Mok of Lingnan University, Hong Kong, but without baseline data that would make it more meaningful.
And interesting, given the large number of Chinese students in Canada, that Canada was not mentioned, along with the importance of health and safety concerns.
Of course, intentions are different than behaviour, and the work that Dan Hiebert, Howard Ramos and I are doing will provide the basis for deeper analysis:
The world is facing an unprecedented health crisis with the spread of COVID-19 across different corners of the globe. Well before the present global health crisis, growing debates have been emerging with regard to the future of internationalisation of education, especially as people begin to question the value and benefits that international education brings. The COVID-19 pandemic again raises the issue of the future of international higher education.
Will COVID-19 adversely affect international education and student mobility? A recent study published by the British Council in April 2020 shows that 39% of Chinese students who were considering studying in the United Kingdom are unsure about whether to cancel their study plans.
China is the largest source of international students in the UK, with 115,014 study visas issued to Chinese students in 2019, representing 45% of international study visas.
When asked about their major concerns regarding overseas learning, the majority of the respondents overwhelmingly rated health and well-being (79%), personal safety (87%), finances (86%) and application difficulties (70%) as their major worries.
Worse still, the international media report a number of cases showing Asian students and residents have experienced discrimination or even assaults when wearing face masks in the UK, Europe and Australia. Such images will have affected Chinese students’ plans and choices for international education.
Studying abroad: Chinese student perspectives
It is against the context of confronting the COVID-19 pandemic that a Lingnan University research team distributed questionnaires to non-local students in Hong Kong and students in mainland China, asking them to share their plans regarding study overseas after the global health crisis.
In addition, we also invited them to indicate their preferred destinations when choosing to study abroad.
The questionnaires were distributed online in late April to early May 2020. By mid-May, we had successfully reached out to around 2,900 respondents and secured 2,739 valid responses after data cleaning.
Hong Kong, as an international metropolis, is also a traditionally popular choice for mainland Chinese students to further their studies.
This survey about Chinese students’ plans for overseas learning was conducted after another survey reported that citizens living in the Greater Bay Area (GBA) in Guangdong province held negative perceptions of Hong Kong earlier in April 2020 following the protests in Hong Kong after the introduction of the Fugitive Offenders amendment bill by the Hong Kong government.
The GBA survey shows people in Guangdong, China, find Hong Kong no longer friendly, safe or well managed in terms of urban governance. Such perceptions will inevitably affect mainland students’ preferences when it comes to making Hong Kong their destination for further studies.
Whether people outside the city perceive Hong Kong as performing well in social management, safety, tolerance and friendliness will have a direct impact on their decisions about studying and working in Hong Kong.
According to our survey about Chinese students’ overseas study plans, most of the respondents (84.4%) said they would choose not to study overseas and only 16% of the interviewees still have plans to study abroad when the global health crisis is over.
When asked about their preferred destinations for overseas learning, the United States remains the most popular destination for study abroad in higher education, followed by Hong Kong.
One point which deserves particular attention is that many of the respondents prefer to study in Asian countries or regions, with Japan and Taiwan being equally popular (on 10.8%), though the UK is rated third (12.2%) among the top five destinations.
The less preferred countries are as follows: France (3.3%), New Zealand (3.3%), South Korea (3.04%), Malaysia (0.94%) and Italy (0.94%).
We found that those students who had previous overseas learning experiences or had enrolled in transnational education programmes through the Sino-foreign cooperative universities based in mainland China showed more interest in pursuing higher degrees through international education.
Among this cohort of students, the intention to study overseas is around 20% higher than among the rest of the survey participants.
Interestingly, Hong Kong is chosen as the second most popular destination by these students.
The above findings are consistent with recent research examining how Chinese students who graduate from UK universities assess the relevance of the overseas learning experiences they received to job acquisition or career development. The present survey again shows the perceived importance of international learning to Chinese students.
Policy implications
Despite the fact that the above data indicate a declining interest in international learning, Hong Kong stands out as a popular destination for those who opt for overseas learning, despite GBA citizens’ concerns about the city being friendly and safe.
A successful world city depends on attracting and retaining world talent. The two surveys draw important policy insights not only for the Hong Kong government but also for society at large. The city is facing unprecedented challenges and concerted efforts are urgently needed to be put together to make Hong Kong competitive and to rebuild its reputation as a friendly and hospitable city for mainland Chinese students.
After fighting COVID-19, academic leaders in Hong Kong need to develop appropriate strategies to attract students from the GBA to come to the city for higher education, seriously engaging with universities in the GBA to promote innovation-centric entrepreneurship.
Our research findings on Chinese students’ choice when planning their international education offer useful policy insights for higher education institutions across different parts of the world, especially when institutions of higher education have relied heavily on Chinese students as one of their major funding sources or incomes.
For small university towns across the UK, Europe, US and Australia, the survey indicates that whether students feel safe and secure will become a major factor influencing their study plans.
Are we ready to embrace internationalisation of education when the COVID-19 crisis is over?
Is it ethical to take in foreign students if local residents are not ready to adapt to diverse understandings and experiences when managing the global health crisis, including the acceptance of ‘wearing face masks’ as a preventive measure?
These are critical issues for us to reflect upon.
Professor Ka Ho Mok is vice president and dean of the School of Graduate Studies and Lam Man Tsan Chair Professor of Comparative Policy at Lingnan University, Hong Kong.
Earlier this year, Jawar Mohammed, the prominent political activist and media entrepreneur, who had returned home to Ethiopia from the US, looked set to challenge his former ally, prime minister Abiy Ahmed, in the country’s election. But there was immediately uncertainty created over Jawar’s eligibility simply because he had been a US citizen. Ethiopian law does not allow dual nationality and even though he written letters saying he’s renounced his US citizenship that uncertainty remains.
Jawar’s case is one of many that highlights an increasingly common issue for many African countries, who after years of battles with Western imperialism and colonial rule were determined at independence for their citizens to literally pick a side and not be allowed to carry the passports of other countries.
But in the 60 years since independence across the continent, the forces of globalization and transatlantic migration has seen dual nationality come up more frequently as an issue which needs to be addressed across politics and business through to sports.
Back in 1985, Saudi Arabia’s soccer authorities initially refused to hand over the trophy of the Afro-Asian Cup after losing to Cameroon in the finals of the tournament. They claimed Cameroon had fielded an ineligible player who was none other than legendary star Roger Milla, who had traveled to Jeddah on a French passport as he couldn’t also have a Cameroonian one.
Now, Cameroon is considering a revision of its nationality code which was enacted in 1968. The current law stipulates any Cameroonian adult who willfully acquires a foreign nationality automatically loses their Cameroon nationality.
But a new draft bill—a copy of which Quartz Africa has seen—says “a Cameroonian who has acquired another nationality shall retain Cameroon nationality unless it is expressly relinquished by the concerned.” The bill is expected to pass through with little challenge.
Some African governments have been reluctant to legalize dual citizenship, arguing the patriotism of people with dual citizenship could be questioned. But there’s also anecdotal evidence some of these governments are more concerned an influential and economically independent diaspora, able to move freely between countries, could support a challenge to the leadership.
Passport limits
By 2010, a comprehensive study showed that 21 African countries, including DR Congo, Liberia, Algeria and Zimbabwe, prohibited dual citizenship. Meanwhile, 23 others permitted dual citizenship under certain circumstances like if acquired by marriage to a foreign spouse or allowed for citizens from birth only. Other countries did not address the issue of dual citizenship in their laws.
Despite these restrictions it is not unusual among middle class Africans to find people holding dual nationality in countries which don’t allow dual nationality, in part because many countries don’t have comprehensive systems for checking until they vie for office. In 2017, up to two-thirds of the presidential candidates in Somalia’s election held foreign passports while as many as 100 of its 275 legislators also held foreign passports. Eventual winner, now president, Mohamed Farmaajo, also held American citizenship. He had previously worked for the state transportation department in Buffalo, New York.
Many African countries today have sizable diaspora communities, notably in Europe and North America, with an increasing economic, social and political influence aided by the improvement in communications and travel networks over the last couple of decades.
The World Bank estimates the African diaspora around the world at 30.6 million, but the figure could be even higher when unrecorded African migrants are considered. In 2019, remittance inflow from the African diaspora topped $48 billion. Such remittances in 2010 contributed to 2.6% of the continent’s GDP.
The IMF has estimated the African diaspora save an around $53 billion every year outside of the continent. There is a belief that if it was easier to invest in their countries of origin as dual nationals more of those savings would come to Africa.
Last year, Ethiopia’s parliament passed a bill to allow members of the Ethiopian diaspora, who have taken up nationalities in other countries, to invest, buy shares, and set up lending businesses in the country’s state-dominated financial sector.
Ghana seems to be one of the African countries which has been quick to recognise the potential of its diaspora and the advantage of granting them the possibility to hold dual citizenship. As early as 2000, it passed a law to recognize dual nationality for its citizens. The government of Ghana has since made efforts to attract its Ghanaian origin and other African descendant diaspora to return home, with the Year of Return, Ghana 2019 recording remarkable success.
Practicalities
Many African professionals and businessmen at home and in the diaspora want to pick up foreign passports for very practical reasons—they want to be able to move freely around the globe.
According to the Africa Visa Openness Report 2019, on average, Africans can only travel to 25% of other African countries without a visa. But holders of passports from North America and Europe can travel visa-free to more African countries than Africans.
Henley & Partners, the global citizenship and residency advisory firm which is set to open an office in Lagos, has pointed out that most Nigerians wishing to subscribe to their offerings have no plans to relocate. Instead, they just want to have a passport which makes it easier to travel without the unpredictability of visa applications.
The latest Henley Passport Index shows that two of Africa’s most populated countries, Nigeria and Ethiopia occupy the 97th and 98thpositions respectively on the index. The Nigerian passport offers its holders visa-free travel to just 46 countries mostly in Africa, while the number is 44 for Ethiopia.